This past September I took NeuroKinetic Therapy (NKT) Level One with Kathy Dooley at Catalyst S.P.O.R.T. NYC. Several of my friends have taken this course and highly recommended it. My philosophy is that knowing more information, having more tricks up your sleeve, and learning new perspectives can only help your patients.
This review is simply my interpretation of the NKT system and how I have tried to incorporate it into my practice. I do not work for NKT or represent NKT. Please visit the NKT website for the authoritative description of the approach.
Kathy Dooley
I want whatever Kathy Dooley has in the morning. She has an insane amount of energy, is extremely knowledgeable, and was very animated during the entire course. She not only has a deep understanding of the NKT approach, but she has mastered it clinically. For me, the best part of the course was watching Kathy perform live demonstrations. These not only displayed the NKT technique, but allowed for a greater understanding of how to incorporate the approach into daily use. She gave a clear, clinical perspective of how she chooses which muscle to “Therapy Localize” and how to incorporate the results of the assessment into your patient’s care.
My favorite Kathy quote:
“I’m not busy because I’m good. I’m busy because I empower my patients.”
Quick Definitions & Semantics
Throughout the course there seemed to be some confusion over some terms and semantics. Hopefully this will help clear things up and make it less confusing.
Here is an oversimplification of the common terms used in the NKT approach:
- Facilitated = On = Strong = Muscle Firing = Neural Drive = Efferent Motor Outflow
- Inhibited = Off = Weak = Muscle Not Firing = No/Minimal Neural Drive
Try not to associate these terms with good or bad. In certain situations you want muscles inhibited. In certain situations you want muscles facilitated. But in this NKT system, you do not want to find a muscle that is so inhibited that it can’t even match a light force. This doesn’t mean inhibition is a bad thing, it just means that muscles should be able to go from an inhibited state to a facilitated state when called upon.
What is NKT?
- “NeuroKinetic Therapy (NKT) is an application of motor control theory, neuroscience, and functional anatomy (neurobiomechanics) that will help you unravel the cause of faulty movement patterns in the brain’s motor control center.” -David Weinstock
NKT gives you another lens through which to view your patients. It uses an innovative manual muscle test coupled with a trial and error of inputs with the goal of improving neural drive.
Here’s the basic progression:
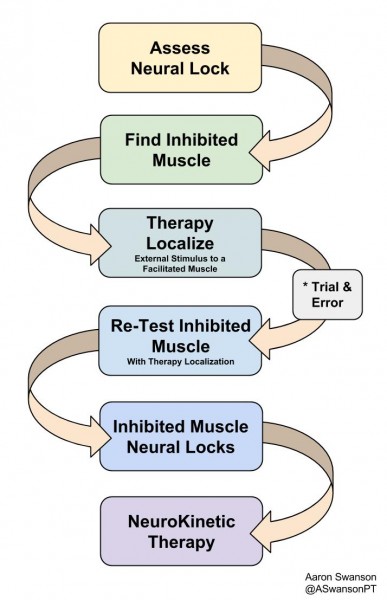
NeuroKinetic Therapy
The main goal is to find a muscle that does not have a Neural Lock. A muscle that can’t even meet a light resistance (inhibited).
The next step is to find a facilitated muscle (a muscle that is already on) to Therapy Localize. Therapy Localization is just when you apply an external input to a “facilitated” muscle while re-assessing the inhibited muscle. It’s simply adding input to change the output, but it’s assessed instantaneously.
Which “facilitated” muscle you pick first to Therapy Localize depends on many factors. It depends on their history, the mechanism of injury or dysfunction, their posture, their breathing pattern, their SFMA breakout, their PRI pattern, their whatever. There are many ways to get to the same place.
The magic happens when you find a “facilitated” muscle that when you Therapy Localize, it turns the inhibited muscle on. Once you find this, you have an input to output response that you can use for the rest of your assessment and treatment. You have a specific muscle to “release” that will faciliate another muscle that needs more neural drive.
After you find this connection the treatment is wide open. You can incorporate a self-release in a circuit. Example: “inhibited” glute max (no neural lock), “facilitated” rectus femoris. Therapy Localization of the rectus femoris results in improved glute max neural drive (neural lock). An example circuit: foam roll rectus femoris, single leg hip thruster, RKC plank, single leg deadlift, repeat (including foam roll at every set). This is just an example – the options depend on your creativity.
This may sound very confusing. But in clinical practice and watching a live demonstration, it becomes much clearer and easier to use.
3 Things I Learned From NKT
1) A New Manual Muscle Test
Traditionally we use manual muscle testing that determines a “specific muscles strength”. However, this doesn’t take into consideration of the complexity of the nervous system. It doesn’t take into consideration the complexity of proximal stability. It doesn’t take into consideration the global system. It doesn’t give you that much information – it tells you if the body can match the random resistance applied from the tester.
In it’s simplest form, NKT is a way to assess the specific neural drive of the musculoskeletal system. It looks at how the nervous system interacts with specific movement patterns. It gives you a specific force, at a specific location, with a specific outcome that relates to the rest of the body.

This is how some people are currently manually muscle testing the biceps
2) The Importance of a Neural Lock

It’s a light touch and the should only meet your pressure, not exceed it (picture idea from Ming Ming Su-Brown)
The overall theme is the same as what some strength and conditioning coaches preach – “you can’t strengthen a muscle that you can’t activate”. In this sense, you are simply looking to see if the muscle is ON (facilitated) or OFF (inhibited). There are graded levels of resistance to assess strength, but the innovation lies in the light touch assessment of the nervous system.
This light touch assessment is simply checking for what they call a “Neural Lock”. It’s the lightest manual muscle test you’ve ever done. You’re simply putting a light force on the body to see if it can “facilitate” the necessary muscles to match the resistance. You’re checking to see if the brain can tell the specific “muscles” to turn on (facilitatie). You’re checking the motor neurons ability to fire from the CNS. You’re not checking strength – you’re checking availability.
An important factor here is that the patient must only “meet your resistance”. I’ve noticed that many go into a high-threshold strategy and over fire all the synergistic muscles to try to make up for the “inhibited” muscle. The light touch shouldn’t be met with a life or death response.
3) A Manual Therapy Assessment
After our manual interventions we often re-assess many different outputs. We assess:
- Pain (depends on an immeasurable amount of variables)
- “How it Feels” (depends on an immeasurable amount of variables)
- Global Movement (depends on many variables)
- Isolated ROM (few variables involved)

How is George going to know what’s really happening if he’s not assessed after the manual technique?
The more variables involved in an output, the more complicated the relationship. This is why re-assessing pain or how it feels may not be the most accurate assessment of your manual skills. It may be more of an assessment of the patients beliefs of your manual skills or your ability to prime the patient, but that’s another story.
Re-assessing a simple input-output relationship, like ROM, gives the practitioner a more accurate way to assess the manual-output relationship.
NKT suggests another simple input-output relationship we should assess – muscle strength/activation. Simply perform manual therapy to “release” a muscle, then re-test a specific muscles strength. You have nothing to lose and specific strength to gain.
For the Critics
I know there are many skeptics out there who will scoff at many of the NKT concepts. I just want to address them here first. If I can turn one pessimistic troll into an inquisitive thinker, then I will consider this a success.
Isolated Muscle Testing
We all know there is no way to truly isolate a muscle without a surgical scalpel. And I’m sure the NKT guys agree. But it’s much easier to say it’s the quadratus lumborium test than the supine lateral flexion with resistance at the ankle test. The specific muscle tests are more about the intention. It’s not meant to disregard to complexity of the connective tissue/fascia system or the nervous system.

Once it hits your lips…
For the global movement people that have a difficult time with non-functional assessments, just consider this as a more specific movement pattern. It’s throwing a load into a system and checking the output. There’s less variables involved with a muscle test compared a complex global movement. This means the outputs measured will be more specific to the chosen inputs. It’s further down the funnel.
If you ask someone to squat (global movement assessment) and their knee caves in it could be a million different things. Specific NKT muscle testing is one of many things you could do that could help you narrow the infinite. It gives more information to help answer the bigger questions.
Facilitated/Inhibiting
We all know muscles are not just off or on. We know we’re not going from full paralysis to full tetany throughout a gait cycle. That said, there is a constant wave of neural drive to assist with movement patterns. We know that some muscles decrease their neural drive and some increase it to accomplish a task. This is a very complex interaction of the body, the environment, and the task.
What NKT does is try to offer a snapshot of a specific area under reproducible constraints. It helps display the variability of a specific, reproducable motor program. It helps narrow the infinit.
Unless you’re Bernie, you don’t have any muscles that are truly off.
Magic
We all know there’s no such thing as magic. But many movement professionals have experienced a drastic change in output from a minimal change in input. Most of the time this chalks up to a temporary neurological response. This temporary neurological response is perceived as magic to people who don’t understand the human body or the nervous system (most of your patients).
Most professionals know this “magic” is not long lasting. It will take many frequent inputs to get it to stick. But for the anxious patient who doesn’t yet buy in to what you’re doing – this is profound. They feel the difference immediately. They don’t have to wait 3-6 weeks to start seeing changes. They don’t have to depend on your manual therapy. They don’t have to change their beliefs. They are given hope. They get excited. Then they buy in and believe everything else you say. Regional interdependence, pain science, and the bodies natural asymmetries are much easier to talk about when the patient already trusts you.
Overall
I enjoyed the NKT class and was happy to learn a new perspective on muscle testing. I have been able to incorporate it into my practice very easily. Similar to the SFMA, the NKT does not remove anything from your practice. It just adds another assessment for more information. You’ll never find what you’re not looking for
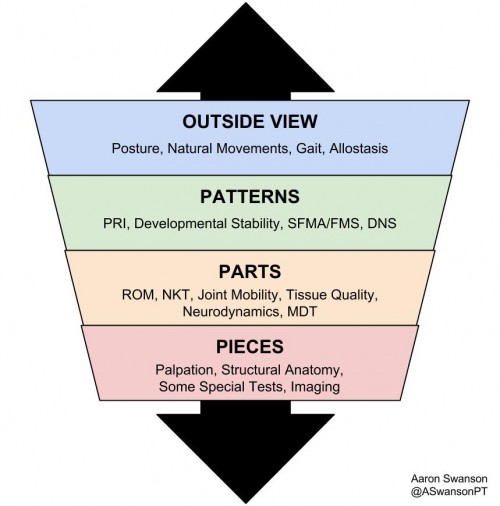
My funnel now and my funnel in college are very different


